
Is the Ebola Epidemic Evolution in Action?
The Ebola epidemic in West Africa has already claimed over 4,000 lives—more than all previous Ebola epidemics combined—and it is showing no sign of slowing. The first (and we hope the only) Ebola death on American soil occurred in Dallas, Texas, on October 8, 2014. Two nurses who cared for that patient, Thomas Eric Duncan, soon developed Ebola. In Spain a nurse exposed in Madrid to a priest who contracted Ebola in Africa recently developed Ebola.1 These incidents represent the first time Ebola has been transmitted outside of Africa.
In the past, outbreaks have remained geographically confined to the regions where the organism that harbors them lives.2 Why is this one different? Is Ebola wielding the power of Darwinian evolution over medical science?
Mr. Duncan’s Case History
The first Ebola victim in the United States, a 42-year-old Liberian citizen, left Liberia symptom free, flew to Texas for his son’s graduation, and developed symptoms five days later. He was seen in the emergency room the next day for fever, vomiting, and abdominal pain. Three days later he returned by ambulance and was diagnosed with Ebola virus.
Ebola symptoms take anywhere from 2 to 21 days to develop. Mr. Duncan may have been exposed to Ebola during the week before his trip while assisting a neighbor, who later died of Ebola.3 Mr. Duncan died two weeks after his symptoms began.4 He shared a Texas apartment with nine people for several days after he developed symptoms. They and 77 hospital staff members have been exposed to Ebola.5 To date, none of the people with whom he lived have developed Ebola,6 but two health care workers, nurses who worked extensively with Mr. Duncan when he was extremely ill and therefore most infectious, have developed fevers and been confirmed to have Ebola.5
What Is Ebola?
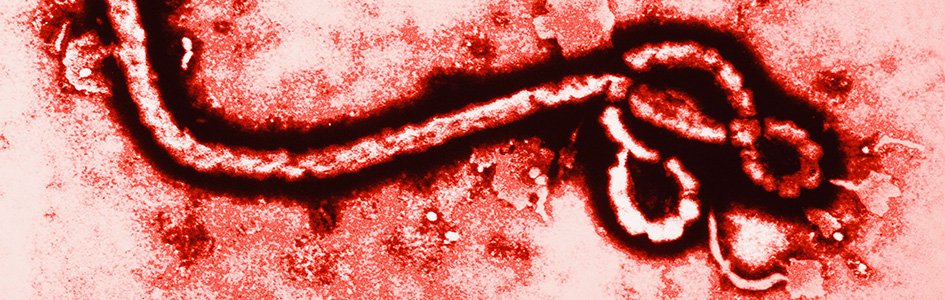
Ebola virus is a stringy bit of RNA in a fatty protein envelope. Like all viruses, it needs the assistance of the cellular machinery in living organisms to replicate itself. A virus either injects its genetic material into a cell or binds to a receptor on the cell surface and is taken in by the cell, which then builds copies of the viral genome and makes more viruses. Generally speaking, symptoms of a viral illness develop when copies of the original virus are released from the cells in which they were built. Certain fruit bats in Africa are thought to harbor Ebola virus. The way the virus is transmitted to humans is unclear, but bats and other types of bushmeat are on the menu in some places that have had outbreaks. Once Ebola infects a person and symptoms develop, any of that person’s body fluids may contain the virus and transmit it to other people. The virus enters through breaks in the skin or through mucous membranes such as the eyes, nose, or mouth. There are thus far no reports of transmission through the air or through touching without body fluid contact.
Early on the symptoms of Ebola, beginning with fever, are pretty much the same as many ordinary viral illnesses: achy muscles, chills, sore throat, headache, nausea, vomiting, diarrhea. This of course makes the disease much harder to diagnose, so medical personnel must be on the alert for viral symptoms in people who have recently traveled in a place where there is an outbreak.
Ebola is one of several viruses that cause viral hemorrhagic fevers.
Ebola is one of several viruses that cause viral hemorrhagic fevers. There are no cures for any of them, largely because the virus tends to mutate very rapidly as it spreads from person to person. Fortunately, not all have a mortality rate as high as Ebola’s, which kills 78% of its victims.7 These hemorrhagic fever viruses differ greatly, even in the organs they attack and the way they cause hemorrhaging. Ebola can attack the liver’s ability to produce clotting factors, for instance, causing a very ill patient to develop leaking and bleeding from many tiny blood vessels throughout the body, leading to shock, shutdown of vital organs, and death. Not all patients develop the hemorrhaging.
There is no cure for Ebola. Though several experimental drugs have been tried, none have been demonstrated to be effective. Apparent “successes” are balanced by failures. Transfusion of antibody-containing serum from a survivor is under investigation, but in Mr. Duncan’s case none with a matching blood type was available.8 Treatment consists of supportive care, which means treating the symptoms with intravenous fluids, oxygen, and even ventilator support and dialysis in the late stages of the disease, until the patient either battles the disease successfully or doesn’t. Because Ebola is transmitted through body fluids, deadly, and incurable, the highest level of isolation precautions are used in caring for patients. And due to the practical realities involved in caring for an extremely sick person, there are many points at which a small and even unnoticed error in strict isolation protocols can lead to tragic exposure and spread the disease further.
Viral Variations
Some have said Ebola is evolving and even suggested it could evolve into an airborne virus.
Like other viruses as well as living organisms, Ebola’s genome can develop variations. The species of Ebola are often named after the country in which they become epidemic. In the past, Ebola outbreaks have been limited to deaths in the hundreds. The death toll in West Africa’s epidemic already exceeds 4,000 and it is expected to rise much higher. The World Health Organization is calling Ebola “the most severe acute public health emergency seen in modern times.”9 Why is this Ebola epidemic so much worse? Some have said Ebola is evolving and even suggested it could evolve into an airborne virus. Is evolution threatening to defeat us?
Though there are obviously many complexities to these questions and many factors yet unknown, readers should see that it is the mathematics of Ebola that threaten worldwide disaster, not Darwinian evolution. When DNA is being copied in a cell, enzymes called “polymerases” do the building, adding nucleotide after nucleotide until all the DNA is copied. Ordinarily, cellular machinery proofreads the DNA it copies, getting rid of most bad copies and keeping the mutation rate low. However, when an RNA virus (like Ebola, or the flu, for that matter) hijacks a cell to make copies of itself, it uses RNA polymerases. These are used in normal human cells to make copies of genes in the DNA in the form of RNA which is then “read” by the cell’s protein factories (ribosomes) to assemble proteins. RNA polymerases don’t proofread very well, so lots and lots of mutations slip through. (This is not a design flaw: For the normal process of making human proteins this isn’t a problem because proofreading is done at an earlier stage.) This is the reason you need a new flu shot every year, because RNA viruses mutate rapidly. In the case of Ebola, the more it spreads, the more opportunities it has to mutate, and the harder it is to treat. Cures and vaccines are difficult to develop when the target keeps changing.
But is this evolution? No. When a virus or microorganism mutates, it might change some of its traits, producing some mutant copies better able to face the challenges in its environment and some less able. Obviously the ones better able to cope survive and become the “parents” of the next generation. But they do not change into different kinds of viruses or microorganisms. Ebola virus remains Ebola virus. This is not an example of molecules-to-man evolution.
Virologists have never seen a non-airborne virus transform into an airborne one in humans.
What about concerns recently mentioned in the news that Ebola could evolve into an airborne virus? Many experts doubt this will occur. Why? Well, even though viruses mutate rapidly, they do not acquire the genetic information to build brand new structures that would make them into a different kind of virus. Virologists have never seen a non-airborne virus transform into an airborne one in humans. Why is that?
Vanderbilt University Infectious Disease specialist Dr. William Schaffner explains why:
We have so many problems with Ebola, let’s not make another one [the possibility of airborne transmission] that, of course, is theoretically possible but is pretty way down on the list of likely issues. Everything that is happening now can easily be comprehensively explained by person-to-person spread via body contact. We don’t have to invoke anything else.
The difficulty is that those viruses don’t have the protein attachments that can actually attach to cells in the upper airway. They have to develop attachments to do that. Since the virus doesn’t have attachment factors that can work in the upper airway, it’s very rare for it to go human to human, and then it almost always stops and doesn’t get to a third person.10
Thus, when we look at the reason many experts believe the virus will not be able to make this leap, we can see it is the distinction between molecules-to-man evolution (which does not happen) and variation within a created kind (which happens all the time) that makes this confidence possible. The fact that organisms are unable to gain new genetic information to add structures and functions leading them to become a different kind of organism, from the human point of view, is a very good thing.
Public Health
In the short time since Mr. Duncan’s death and the Ebola transmission to his nurses, many Americans have been gripped with fear. It is vital to follow the procedures recommended by the CDC in any situation in which there is a legitimate risk of exposure. However, there is no evidence that the virus is transmitted through the air or by touching hard surfaces or through any avenue other than direct contact with body fluids from a person with a symptomatic infection. Regarding concerns about air travel, and in particular a commercial flight on which one of the sick nurses flew with a temperature of 99.5 degrees Fahrenheit, Dr. Schaffner told NBC Nightly News that people need not be fearful of contracting Ebola from such casual contact:
I would be perfectly comfortable today if I had sat right next to her. My risk of acquiring Ebola infection is really zero.11
University of Pittsburgh Medical Center Infectious Disease specialist Dr. Amesh Adalja, a recognized expert in pandemic preparedness,12 told NBC,
The general public need not panic. Ebola is not spread through casual contact. You can’t get it on the subway. People aren’t walking around with Ebola in your neighborhood.11
Because symptoms usually start with fever, the CDC has recommended airports screen passengers traveling from West Africa for fever. CDC officials admit that this procedure probably would not have detected Mr. Duncan, however, as he was symptom free on arrival. Dr. Martin Cetron, director of the CDC’s Division of Global Migration and Quarantine, admits, “No matter how many of these procedures are put into place, we can’t get the risk to zero.”13
What about health care facilities? What can we do to safely care for Ebola patients without spreading it further? Why did the nurse in Texas get exposed? What about health care workers exposed in Africa? CDC director Dr. Tom Frieden says, in the case of Mr. Duncan, there must have been a “breach of protocol,” and the CDC is investigating the situation and planning to ramp up the infection control training for healthcare workers.14 Dr. Frieden says that we have decades of experience caring for people with Ebola and know the isolation protocols work, though they are extremely difficult to follow perfectly.14 Notably, the CDC director says that simply increasing the amount of personal protective equipment workers wear is not the answer to the problem, as cumbersome gear makes it even more difficult to care for patients safely. The CDC is evaluating the isolation procedures in place at the hospital as they work to determine how biocontainment protocols were compromised. Dr. Frieden is confident that in this country the CDC’s procedures for tracking down and monitoring contacts of Ebola patients closely for 21 days, coupled with isolation of any who develop symptoms, will be successful in preventing a massive epidemic.14
Must We Know Ebola’s Evolutionary History to Fight It?
Update November 1, 2014
Evolutionary biologists believe they can track the evolution of filoviruses and the animals into whose genomes they have been incorporated. Recent reports assert, “Filoviruses are far more ancient than previously thought. These things have been interacting with mammals for a long time, several million years,” University of Buffalo biologist Dr. Derek Taylor says in UPI’s Science News column.
As Dr. Fabich mentioned in “Where Did Ebola Come From?,” the genomes of many different animals harbor the Ebola virus genome. Whether and how this is related to the emergence of infection in humans is still under investigation. The same is true of Marburg virus, another filovirus very similar in structure and infectious behavior to Ebola. In a study published in PeerJ, Taylor and colleagues write, “An understanding of the timescale of evolution is critical for comparative virology but remains elusive for many RNA viruses. . . . For example, ebolaviruses and marburgviruses are well-studied mammalian pathogens, but their comparative biology is difficult to interpret because the existing estimates of divergence are controversial.”15
Research has shown, for instance, that although the genomes of Ebola virus and Marburg virus are very similar, elements from two of the genes that are unique to Ebola appear in some rodents (mice and rats) but not others. The researchers admit these genes, which are found in similar locations in the genomes of living animals, are not “real fossils.”16 They call them “fossil genes” because they might reveal something about the way the host animal species are related. Estimates of how long ago the genes were incorporated into the host genome are based on the worldview-dependent assumptions and circular reasoning applied to the actual fossil record and to molecular clock dates.
Hence, some thought Ebola virus was about 13 million years old, an age reflecting evolutionary beliefs about when those particular rodents diverged. Now they have found that genetic elements common to both viruses are found in other rodents (voles and hamsters) believed to have diverged from a common ancestral rodent 23 million years ago. They therefore believe the ancestor of Ebola and Marburg viruses evolved and infected this ancestor at least 23 million years ago.
While tracing the variations in viruses and microbes is an essential part of dissecting their pathogenesis and getting clues to therapeutic approaches, researchers are not seeing evidence that these viruses or their animal hosts have evolved in the molecules-to-man sense. Filoviruses like Marburg virus—which showed up in Marburg, Germany, in workers handling green monkeys—and Ebola virus are very similar genetically and structurally and are therefore considered to belong to the same family and therefore to be variations descended from the same original type of virus.
Furthermore, the presence of viral genes in various animals—such as different species of rodents—may represent the footprints of their speciation, which is a form of variation within created kinds. But such speciation also has nothing to do with molecules-to-mouse evolution. Since viruses would have been a harmless part of God’s original good creation, it is not surprising to see that they have a long history. But to assign dates of 13 million or 23 million years to the time of their divergence is merely to take the assumption-ridden dates assigned to the divergence of various species of rodents (in the PeerJ study) and imply that they have clinical significance. They do not. Research such as this should be helpful in identifying any animals that might be the source of human infection and hopefully then the mechanism by which the virus spread to humans. But that has nothing to do with millions of years of molecules-to-mouse evolution.
Why Did God Make Viruses?
We constantly point out that God created a very good world (Genesis 1:31) unmarred by suffering and death until after man sinned against God. We know from Genesis 1 that God made all kinds of living things and that they only vary within their created kinds. And while viruses are not technically alive, they are clearly part of the created world. In the face of the current crisis in Africa and potentially around the world, some might ask why God made viruses. Because we are confident that the original world was good until the curse of man’s sin fell upon it, we know that the original viruses—like the original kinds of bacteria and all other microorganisms—must have been harmless and served useful purposes. Over the past 6,000 years many disease-causing variations have developed in viruses and indeed in all classes of microbes. However, the more science learns about this hard-to-see part of our world, the more hints we see that these things were designed as a vital part of our world. You can read more about these in the articles below, and in microbiologist Dr. Andrew Fabich’s latest article “Where Did Ebola Come From?”
Ebola is indeed the latest challenge in this sin-cursed world, and a very dangerous one. But it is not powered by Darwinian evolution.
Ebola is indeed the latest challenge in this sin-cursed world, and a very dangerous one. But it is not powered by Darwinian evolution. And as with every challenge faced by medical science, the battle against it is being fought with observational science and compassionate human beings willing to put themselves at risk to care for the sick.
This information is intended for general education purposes only and is not intended as professional medical advice. The information should not be relied upon as a substitute for medical advice from your doctor or other health care professional. If you have specific questions about any medical condition, diagnosis, or treatment, you should consult your doctor or other healthcare provider or go to a hospital.


Footnotes
- Doug Stanglin, “Spanish Nurse Infected with Ebola After Treating Priest,” USA Today, October 6, 2014, http://www.usatoday.com/story/news/world/2014/10/06/ebola-spanish-nurse-sierra-leone/16816465/.
- The viruses that cause viral hemorrhagic fevers are all dependent on an animal or insect as a natural reservoir, and they are typically restricted geographically to the places where that host species lives. In the case of Ebola and the similar Marburg virus, the host organism is uncertain, though a fruit bat is suspected. For more information, see “Viral Hemorrhagic Fevers,” Centers for Disease Control, last modified June 19, 2013, http://www.cdc.gov/ncidod/dvrd/spb/mnpages/dispages/vhf.htm.
- “CDC Director: Second Case of Ebola in US Result of ‘Breach of Protocol,” Fox News, October 12, 2014, http://www.foxnews.com/health/2014/10/12/health-care-worker-at-dallas-hospital-tests-positive-for-ebola/.
- Associated Press et al., “Ebola in America: A Timeline of Thomas Eric Duncan’s Demise,” The Grio, October 11, 2014, http://thegrio.com/2014/10/11/ebola-in-america/.
- Stan Schroeder and Amanda Wills, “‘It May Get Worse Before It Gets Better’: Second Ebola Case in Texas,” Mashable, October 15, 2014, http://mashable.com/2014/10/15/second-health-care-worker-tests-positive-for-ebola-in-texas/.
- Today marks the end of the 21-day isolation period for Mr. Duncan’s fiancée and others who were in close contact with him before he was taken by ambulance to the hospital. None of them have become ill.
- Reports vary between 50% and 90%. Currently the “average case fatality rate” is 78%. From S. Gire et al., “Genomic Surveillance Elucidates Ebola Virus Origin and Transmission During the 2014 Outbreak,” Science 345, no. 6202 (September 12, 2014): 1369–1372, 10.1126/science.1259657.
- Faith Karimi and Catherine E. Shoichet, “Thomas Eric Duncan: 7 Ways His Ebola Case Differs from Others in U.S.,” CNN, October 10, 2014, http://www.cnn.com/2014/10/09/health/ebola-duncan-death-cause/index.html.
- Evan Horowitz, “How the Ebola Outbreak Spun Out of Control,” The Boston Globe, October 8, 2014, http://www.bostonglobe.com/news/world/2014/10/08/how-this-ebola-outbreak-spun-out-control/b3Fea51l1oRs4c0gjN36EM/story.html.
- Mary Chastain, “Experts Worry Outbreak Could Trigger Ebola Evolution into Airborne Virus,” Breitbart, October 3, 2014, http://www.breitbart.com/Big-Peace/2014/10/03/Experts-Worry-Outbreak-Could-Trigger-Ebola-Evolution-into-Airborne-Virus.
- “Ebola Fear Running Rampant In Many Communities,” NBC News, October 17, 2014, http://www.nbcnews.com/watch/nightly-news/ebola-fear-running-rampant-in-many-communities-344337987872
- “Amesh A. Adalja, MD, FACP,” UPMC, accessed October 20, 2014, http://www.ccm.pitt.edu/directory/profile/amesh-adalja-md-facp
- Jen Christensen, Joe Sutton, and Ray Sanchez, “Ebola Screenings Begin at JFK; Four More Airports Start Next Week,” CNN, October 12, 2014, http://www.cnn.com/2014/10/11/health/ebola/index.html.
- See video at “CDC Director: Second Case of Ebola in US Result of ‘Breach of Protocol,” Fox News, http://www.foxnews.com/health/2014/10/12/health-care-worker-at-dallas-hospital-tests-positive-for-ebola/.
- From D. Taylor et al., “Evidence that ebolaviruses and cuevaviruses have been diverging from marburgviruses since the Miocene,” PeerJ (2 September 2014), https://peerj.com/articles/556/.
- From D. Taylor et al., “Evidence that ebolaviruses and cuevaviruses have been diverging from marburgviruses since the Miocene,” PeerJ (2 September 2014), https://peerj.com/articles/556/. The UPI article erroneously states that the researchers analyzed “genetic material left behind by the virus in animal fossils,” but the scientists make no such claim.

Support the creation/gospel message by donating or getting involved!

Answers in Genesis is an apologetics ministry, dedicated to helping Christians defend their faith and proclaim the good news of Jesus Christ.
- Customer Service 800.778.3390
- Available Monday–Friday | 9 AM–5 PM ET
- © 2026 Answers in Genesis