
Organ Recital: A Parade of Presumed Design Flaws Devoid of Truth
Health column blames our propensity for physical problems on faulty body design, but evolutionary presuppositions obscure the real facts.
Mr. Potato Head’s parts do what they’re designed to do. This illustration accompanies an article proclaiming that the human body is full of design flaws and that “Nature” should take many of our body parts “back to the drawing board.”1
A survey of health columnist Lucy Elkins’s recent articles in the Daily Mail reveals a number of practical tips about common viral illnesses, health risks in your kitchen sink, and why fat puppies aren’t really cute. These articles are useful because they are based on the practical applications of experimental, observational, here-and-now science. But her most recent column, “From eyes in the wrong place to a belly full of bugs: The bits of your body that NATURE got wrong”2—colorfully illustrated with Mr. Potato Head plaintively offering the final word on body parts—fails miserably, largely because it is based on evolutionary presuppositions.
Elkins writes, “faulty body design often makes us prone to illness. Here, the experts reveal the body parts that, ideally, should go back to the drawing board.” Following is a catalogue of body parts she says we’d be better off without. Some are popularly presumed to be useless vestigial evolutionary leftovers. Others she treats as the products of evolution that have outlived their usefulness or failed to keep up with our changing environment. In addition to presenting incorrect conclusions based on evolutionary assumptions, she fails to point out the positive functional designs of the body parts she derides.
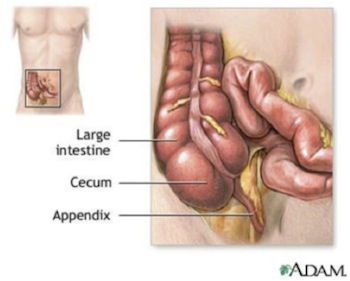
The appendix is located at the juncture of the small intestine and the first part of the large intestine, called the cecum. Despite the common assertion that the appendix is a useless evolutionary vestige, comparative primate anatomy cannot trace its supposed origin. And despite the fact that we can live without it, it actually serves important functions in the immune system.3
The appendix leads the parade of parts as Elkins trots out the tired and outdated notion that the appendix has “no real function.” In reality, however, the appendix not only produces many chemicals that control biological systems in the human embryo, it also continues to fill a number of helpful roles in the development of the immune system in the early decades of life. By exposing white blood cells to antigens in the local environment of the digestive tract, those cells are prepared for their important jobs of antibody production.4 Thanks to modern research revealing the appendix’s important functions in the immune system, most doctors no longer routinely remove healthy ones, despite Elkins belief that it would be “simpler to get rid of it.”
Finding flaws with the way teeth are attached to our jaws is next in line. The problem Elkins points out is that the space between the soft gums and hard teeth allows bacteria to penetrate, leading to periodontal disease. Quoting Dr. Margaret Kellett, dental director of Leeds Dental Institute, she writes, “Really, it would have been better if teeth were anchored into a harder, more bone-like structure which bacteria could not penetrate so readily.” While the importance of using good dental hygiene and avoiding processed sweets to maintain good gingival health cannot be overestimated, we should consider a boney alternative to the excellent design of the periodontal ligament with great caution.
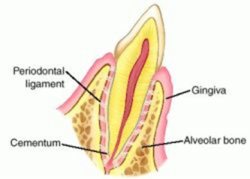
The periodontal ligament is a continuation of your gums into the invisible place between your tooth roots and your jawbone. It is a shock absorber. It is also the home of many types of cells needed to nourish and maintain both the cementum of the teeth and the boney tooth sockets in the jaw.5
The periodontal ligament is a continuation of the visible part of your gums. It dips down to wrap your tooth roots, and it forms a tough but pliable connection between the tooth and jaw. The periodontal membrane is thus a shock absorber, providing each tooth with a bit of “give” as you chew or even clench your teeth. But it does much more than take a pounding with every bite. The periodontal ligament is the home of the many types of cells that build the bone of the socket and the cementum of the tooth, and it is attached to both. “These cells are all important in the dynamic relationship between the tooth and the bone,” according to endodontist Dr. Jason Hales.6 Thus without this shock absorbing toolkit for tooth and bone health, there would be no dynamic interface to allow for the gradual eruption and growth of teeth. So floss and brush, forget the sweets, and be thankful those jawbreaker candies you used to crunch didn’t really break your jaws.
What about wisdom teeth? Once again, Elkins cites Kellet’s evolutionary explanation for why so many people don’t seem to have room for their wisdom teeth nowadays. Kellet says, “Our cavemen ancestors ate predominately raw meat and vegetation, which required a lot of force to chew.” But thanks to soft cooked foods, “the muscles around the jaw need to exert less force on it — causing it to shrink over the years. However, our teeth have not evolved at the same rate, so we are left with a smaller jaw but the same amount of teeth.”
Well, cavemen were just people, and even in the Middle Ages most people still seemed to have room in their mouths for their wisdom teeth. Furthermore, wisdom tooth problems are more prevalent among certain people groups and seem to be associated with more a more complex array of differences than just jaw size. Some researchers now question the value of their routine prophylactic removal. Modern research suggests that the complex relationship between the jaw and teeth is affected by numerous factors, such as genetic differences like mutations, improper dental hygiene, and the impact of diet on jaw growth during childhood. But to ask why our teeth have not de-evolved fast enough to lose these much-maligned teeth begs the question of how they could have evolved in the first place. There is also no reason to think the presence of an anatomical feature that many people can do without means it was a bad design in the first place. (See Are Wisdom Teeth (Third Molars) Vestiges of Human Evolution? and Is Lack of Room for Wisdom Teeth Proof of Evolution? for more wisdom about wisdom teeth.)
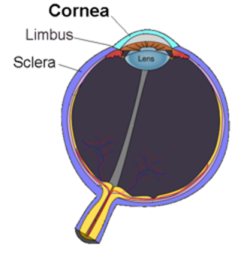
The extreme curvature of the cornea causes it to protrude out in front of the eyeball, making it vulnerable to injury. But that curvature is essential, providing two-thirds of the eye’s focusing power. The adjustable part of the eye’s focal ability comes from the lens. The lens adds layers, growing throughout life. After about age 20, it becomes rounder, but it normally continues to accommodate quite well for decades. The cause of its stiffness in later life, as well as an understanding of all the factors involved in the development of presbyopia as we age, are not yet understood.7
Our eyes also stick out too far, Elkins says. Citing London surgeon David Gartry’s evolutionary spin on why corneal injury is common, she writes, “We evolved like this so that we could scan for predators and prey. … A deeper set eye would have been preferable.”
The cornea curves outward and protrudes a bit in front of the rest of your eye. Of course, some part of you has to take the “point position,” so why not the part that can gather visual information, an important function even when we’re not stalking our dinner? Furthermore, a deeper set for our eyes would decrease our field of vision, which would probably increase motor vehicle fatalities even if Dr. Gartry doesn’t think we need to be on the lookout for predators. The extreme corneal curve is also essential to its function because the cornea provides two-thirds of the eye’s focusing power.
Elkins says an additional “design flaw” is the eye’s lens. With age, the lens tends to get stiffer, decreasing its ability to accommodate for close-up focus. This is called presbypopia. Gartry blames presbyopia on the fact that the lens continues to grow throughout life, adding layers and getting too thick. But the cause of presbyopia is actually a matter of great debate among experts, and to blame it on the fact that the lens grows is short-sighted. The problem is thought to be multifactorial and likely includes deterioration in the lens proteins themselves and in the surrounding muscles that adjust the lens.8
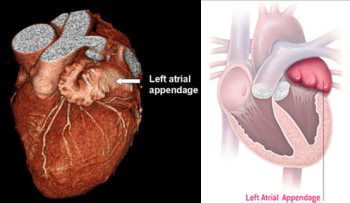
The left atrial appendage is an outpouching of the left atrium, which is located just beneath it in the photograph and diagram. Far from being a bad design or a useless evolutionary leftover, it’s anatomical location and the structure of its wall make it ideally suited as a decompression chamber for the left atrium, protecting the latter from high pressures generated when the ventricles contract. It is also equipped to monitor blood pressure and to respond with chemicals that affect vessels all over the body as well as the amount of sodium the body retains.9
Next, the heart catches grief for its left atrial appendage. This wrinkle-walled little pocket hanging off the left atrium is what remains of the embryonic heart’s original left atrium, the final version of the left atrium being formed as a smooth-walled expansion of the pulmonary veins. Elkins quotes cardiologist Amanda Varnava, saying, “It is completely redundant — it has no functional role. However, if someone has poor circulation, then blood can pool there. When this happens, it is easy for clots to form and cause a stroke.”
A substantial percentage (about 90 percent) of the atrial thrombi (clots) that lead to strokes in patients with atrial fibrillation do originate from blood pooled in the left atrial appendage.10 The primary problem in these patients is their atrial fibrillation, a heart arrhythmia, not the anatomical design of their hearts. But even apart from evolutionary speculations, if clots can develop in it during atrial fibrillation, did God produce a poor design by allowing the left atrial appendage to persist? Does it serve any useful purpose?
The left atrial appendage, it turns out, is neither an evolutionary leftover nor a design flaw on God’s part. It is also not “completely redundant.” If you do not develop atrial fibrillation, your left atrial appendage will likely help you far more than it will ever hurt you. Because of its wrinkled walls and its anatomic position, the left atrial appendage functions as a “decompression chamber” for the left atrium itself, protecting it as the heart generates tremendous pressures with each beat. In addition, it is equipped with stretch sensitive receptors and a generous supply of chemicals that, when released, trigger protective responses (vasodilation and sodium excretion) in response to high blood pressure.11 Thus, the left atrial appendage serves not only an embryonic function but also an important hemodynamic function throughout life.
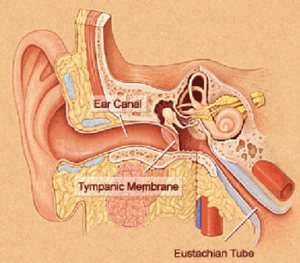
The Eustachian tube connects the middle ear to the nasopharynx, which is located behind your nose and above your throat. The Eustachian tube is very narrow and is supposed to remain closed until it needs to open to equalize pressure between the middle ear and the atmosphere. Watch the short series of illustrations at http://www.dizziness-and-balance.com/disorders/symptoms/etdysfunction.htm to see a graphic demonstration of how this system normally functions.12
What about the Eustachian tubes—those small-caliber tubes that connect your middle ear to your nasopharynx (just above your throat)? They are designed to equalize the air pressure behind the eardrum (where your tiny ear bones are located) and the atmosphere. When those pressures are not equalized—as happens temporarily on an airplane during takeoff—it is difficult to hear. When they get clogged with mucous, trapped fluid in the ear may also get infected. So is this a design flaw? Elkins indicates they are too narrow.
Well, had God made them larger, fluids and bacteria would have reached the middle ear more easily. (This is the reason babies who are fed with a propped up bottle frequently get lots of ear infections.) You also would hear your own voice echoing as if you were in a barrel and be disturbed by hearing your own heartbeat and breathing amplified—a condition that occurs in people afflicted with chronically open Eustachian tubes. In fact, the caliber of the Eustachian tubes needs to be small—so small that they remain closed until pressure differences or the need to drain mucous from the middle ear prompt them to open. The fact that having a cold can make them swell and drain poorly can be said of the entire upper respiratory system, but getting a respiratory infection is a result of living in a sin-cursed world. It does not reveal a flaw in God’s original design.
The article in the Daily Mail also indicates the delicate hair-like sensory structures in the ear’s cochlea are a poor design because they can be irreparably damaged by an extremely loud explosion or chronic exposure to loud noise.13 We might as well call gravity a design flaw because falling off cliffs kills people. The structures are not designed to regenerate, but then we weren’t designed to have our hearing blasted away by loud explosions and dangerously high-decibel music either.
The nervous system is deemed flawed because pain that warns us to stop doing whatever hurts may be out of proportion to the threat. Then again, if pain is designed to discourage us from doing things that hurt, shouldn’t the pain be sufficient to prove a real deterrent? An additional flaw is implicated because permanently damaged tissues may suffer from chronic pain. But injuries and permanent damage to our bodies are the result of living in a sin-cursed world. The pain they cause is not therefore a result of poor design.
Cartilage—the connective tissue that cushions our joints—is described as a flawed design too. Why? Cartilage has no blood supply of its own and therefore may heal poorly when injured. But what would happen if joint cartilage contained a rich supply of blood vessels instead of relying on vessels safely ensconced in adjacent bone? With constant grinding in our joints, those delicate vessels would surely be crushed, bleeding painfully into the joint spaces. While we would all like to have joints that don’t degenerate with age and injuries, the design of joint cartilage—lubricated by synovial fluid and nourished by blood vessels protected in bone—is a good one.
How about reflux esophagitis, the unfortunate result of burping stomach acid up past the gastro-esophageal valve? If that happens chronically, the delicate lining of the esophagus can be damaged, so the author considers that valve to be too loose—a bad design. But gastroenterologist Chris Hawkey rightly points out that if the valve were tighter, we wouldn’t be able to swallow. Furthermore, the valve is not designed to be weak, so chronic acid reflux tends to be a problem when the valve is abnormally weak or when a person is overweight. Neither of these is part of the design.
Finally, the large intestine comes under fire. Besides absorbing the water as one of the final functions of the digestive tract, the colon is home to a lot of bacteria (gut flora) that break down some of the dietary fiber that passes through, yielding 20–30 calories per day—an evolutionary advantage during tough times according to Hawkey. But those bacteria can get out of control and cause problems, so Elkins writes, “We could do without the bacteria and all the problems they can cause.”
Elkins seems to be unaware of even the most basic vital functions of the gut flora. In addition to manufacturing vitamins (vitamin K and biotin) for us, discarded gut flora typically comprise up to 60 percent of the bulk of fecal material.14 Bulk is important in the process of moving waste products efficiently through the colon, as too slow a transit allow toxic materials to be reabsorbed into the body. The gut flora are also friendly colonists that by their very presence ordinarily prevent the overgrowth of harmful microbes. Furthermore, these bacteria play a role in our normal immune responses and have a positive effect on the mucosal lining of the normal colon. One journal article has described the gut flora as the “forgotten organ,” virtually “an organ within an organ.”15 The presence of bacteria in the colon is certainly no design flaw.
God did design a perfect human body along with a perfect world in the beginning.
So what is the alternative explanation? While space here does not permit us to even brush the surface of these intricate designs, the human body is indeed wonderfully created—so why does so much go wrong with it? God did design a perfect human body along with a perfect world in the beginning. How do we know? He told us so in Genesis 1:31, “Then God saw everything that He had made, and indeed it was very good.
”
Adam, Eve, and all their children would have been able to live forever without death and disease had our first parents not chosen to rebel against their Creator. The Curse for man’s sin was no surprise. God warned Adam about it beforehand (Genesis 2:16–17). Ever since the day man rebelled against the Creator, the entire world has groaned under sin. People’s bodies have worn down, gotten ill, and died. Many microbes, designed to be beneficial components in God’s created world, even became the causes of disease. The list of these diseases includes those Elkins blames on “bad design.” The Curse does not show that God’s original designs were bad. The “fault” is not with the Creator—the fault is with mankind. We should rather be thankful that our bodies work as well as they do, that our immune systems protect us from the vast majority of threats, and that the phenomenal process of embryologic development usually operates as it should. We are truly “fearfully and wonderfully made
” (Psalm 139:14).
For more information:
- Vestigial Hiccups, Folding Fish-eyes, and Other Fables: Our Fishy Forebears . . . Again!
- The Human Vermiform Appendix
- The Seeing Eye
- The Hearing Ear
- Cutting Out a Useless Vestigial Argument
- Are Wisdom Teeth (Third Molars) Vestiges of Human Evolution?
- Is Lack of Room for Wisdom Teeth Proof of Evolution?
- (bowel bug types)
- Homo erectus Grew Teeth Like Modern Humans, Not Like Chimps (molar roots and our roots)
- Good Designs Gone Bad
- Microbes and the Days of Creation
- The Role of Genomic Islands, Mutation, and Displacement in the Origin of Bacterial Pathogenicity
- The Genesis of Pathogenic E. coli
- Robert Koch, Creation, and the Specificity of Germs
- Antibiotic Resistance of Bacteria: An Example of Evolution in Action?
- All Creatures Great & Small (DVD)
- The Hearing Ear and the Seeing Eye (DVD)
- Body of Evidence (DVD Set)
- Darwin vs. the Eye
- My Bionic Ear
- A Possible Function of Entamoeba histolytica in the Creation Model
This information is intended for general education purposes only and is not intended as professional medical advice. The information should not be relied upon as a substitute for medical advice from your doctor or other healthcare professional. If you have specific questions about any medical condition, diagnosis, or treatment, you should consult your doctor or other healthcare provider.

Footnotes
- Image credit: Soleman Workshop through http://www.dailymail.co.uk/health/article-2273438/From-eyes-wrong-place-belly-bugs-The-bits-body-NATURE-got-wrong.html
- http://www.dailymail.co.uk/health/article-2273438/From-eyes-wrong-place-belly-bugs-The-bits-body-NATURE-got-wrong.html
- Image credit: University of Maryland Medical Center http://www.umm.edu/patiented/articles/appendix_000170.htm
- http://www.scientificamerican.com/article.cfm?id=what-is-the-function-of-t
- Image credit: http://www.theendoblog.com/2011/11/who-cares-about-periodontal-ligament.html
- http://www.theendoblog.com/2011/11/who-cares-about-periodontal-ligament.html
- Image credit: http://en.wikipedia.org/wiki/Cornea
- http://onlinelibrary.wiley.com/doi/10.1046/j.1475-1313.1995.9500095u.x/abstract
- Image credit: photograph from National University Heart Centre, Singapore http://www.nuhcs.com.sg/patients-and-visitors/our-services/cardiology/transcatheter-left-atrial-appendage-closure.html and diagram from http://www.bostonscientific.com/watchman-eu/assets/images/sub-pages/therapy-watchman-235x340.jpg
- N. Al-Saady et al., “Left atrial appendage: structure, function, and role in thromboembolism,” Heart (1999) 82:547-555 http://heart.bmj.com/content/82/5/547.full
- N. Al-Saady et al., “Left atrial appendage: structure, function, and role in thromboembolism,” Heart (1999) 82:547-555 http://heart.bmj.com/content/82/5/547.full
- Image credit: Northwestern University and Timothy C. Hain, M.D. at http://www.dizziness-and-balance.com/disorders/symptoms/etdysfunction.htm
- The Hearing Ear
- Though the more commonly quoted figure for the proportion of dead bacteria in solid fecal material is 30 percent (as in J. Hall, Guyton and Hall Textbook of Medical Physiology 12th edition, Philadelphia: Saunders, 2011, page 798, for instance), this figure is generally based on counting the bacteria in samples, assuming an average figure for the size of bacteria, and calculating the weight. A more direct method of assessing the bacterial mass involves separating the microbial mass from the undigested fiber and soluble components and actually weighing the bacteria. A study using this method to evaluate healthy British volunteers found that the true microbial contribution was 60 percent, about double the commonly quoted figure. Naturally, as the researchers also noted, the actual figure could vary greatly depending on dietary fiber intake. (A. Stephen and J. Cummings, “The Microbial Contribution to Human Faecal Mass,” Journal of Medical Microbiology (1980) 13:1, pages 45–56. jmm.sgmjournals.org/content/13/1/45.full.pdf+html)
- http://www.nature.com/embor/journal/v7/n7/full/7400731.html
Support the creation/gospel message by donating or getting involved!

Answers in Genesis is an apologetics ministry, dedicated to helping Christians defend their faith and proclaim the good news of Jesus Christ.
- Customer Service 800.778.3390
- © 2025 Answers in Genesis